
Epidural injections deliver a combination of "local anesthetics and steroids" directly to the inflamed nerves, reducing inflammation and swelling while blocking pain signals. This treatment is suitable for radiating pain associated with conditions such as herniated discs, sciatica, and spinal stenosis. When guided by X-ray or ultrasound, the procedure is even more precise and safe.
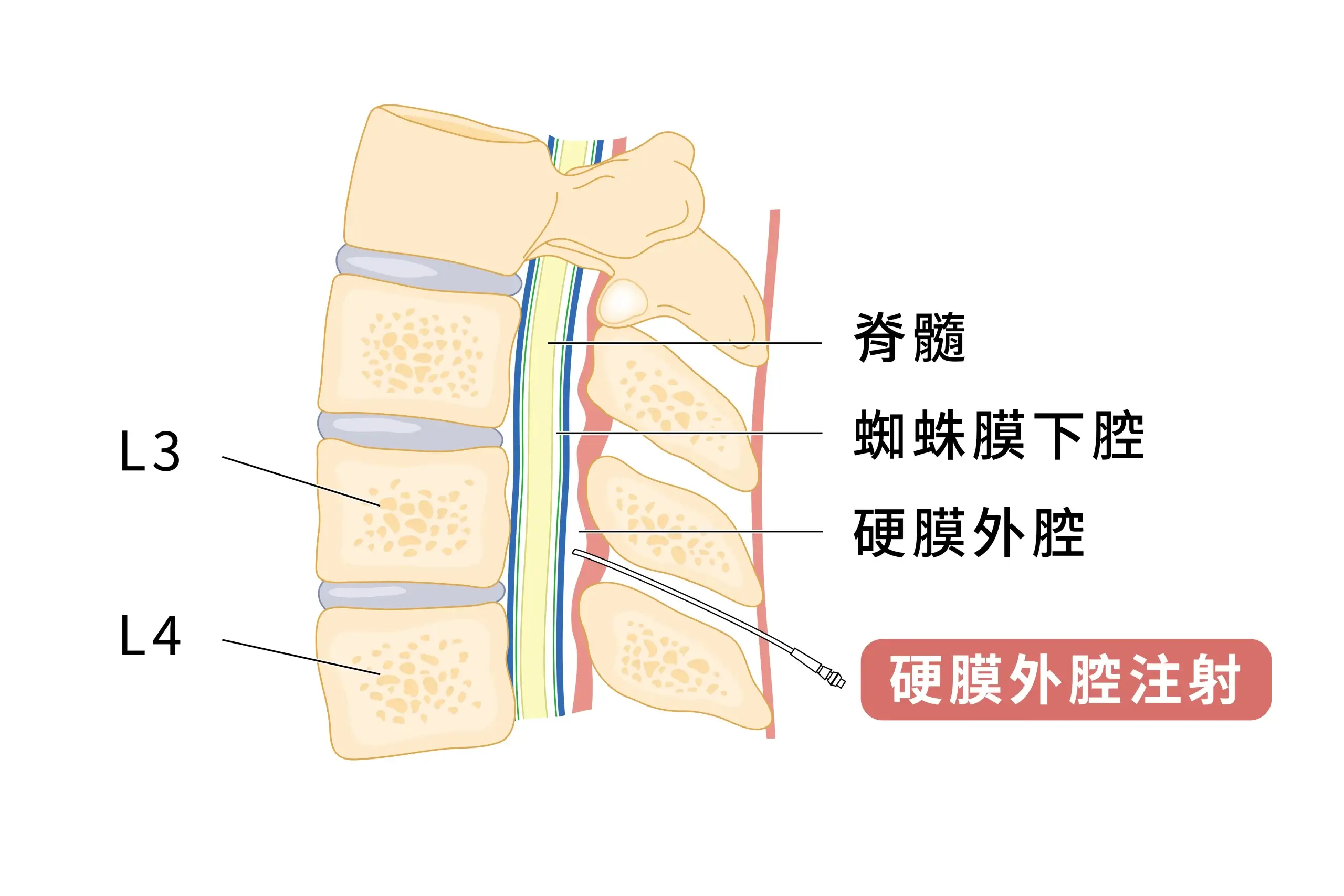
The epidural space lies between the spinal cord and the bony structures of the spine. It contains fatty tissue, blood vessels, lymphatic vessels, and nerve roots. An epidural steroid injection (ESI) involves injecting a mixture of local anesthetic and steroids into the epidural space, where it acts directly on the area surrounding the inflamed nerve. The primary objectives are:
- Reduce nerve swelling and inflammation
- To reduce the transmission of pain signals
- To alleviate symptoms such as sciatica and herniated discs
The procedure is typically performed in the lumbar or thoracic spine and is guided by X-ray or ultrasound to enhance safety and precision. In most cases, ESI is used as a short-term adjunct for pain relief and can serve as a bridging option between conservative treatment and surgery.






