Caudal Epidural Injection

Regen Health
2025-11-27
What if rehabilitation is ineffective? Learn about "Caudal Epidural Injection": a rescue technique that is more direct than traditional painkillers and safer than surgery.
Faced with sciatica that feels like an electric shock to the toes, or lower back pain that persists even after six months of rehabilitation, many people’s first instinct is: “Do I really need surgery?” We completely understand this anxiety of struggling between pain and the risks of surgery.
In fact, between ineffective medication and surgery, modern pain medicine offers a more precise and relatively safer option—”Caudal Epidural Injection.”
This technique doesn’t actually “sever” the nerve. Instead, it uses advanced imaging guidance (such as ultrasound or X-rays) to precisely deliver a tiny amount of medication to the point of nerve compression, much like a fire brigade. It not only effectively removes inflammatory substances and relieves severe pain, but also helps many patients who have long suffered from lower back pain regain their dignity in walking and daily life.
What is a Caudal Epidural Injection?
Caudal Epidural Injection is a minimally invasive regional treatment for lower back and pelvic pain.
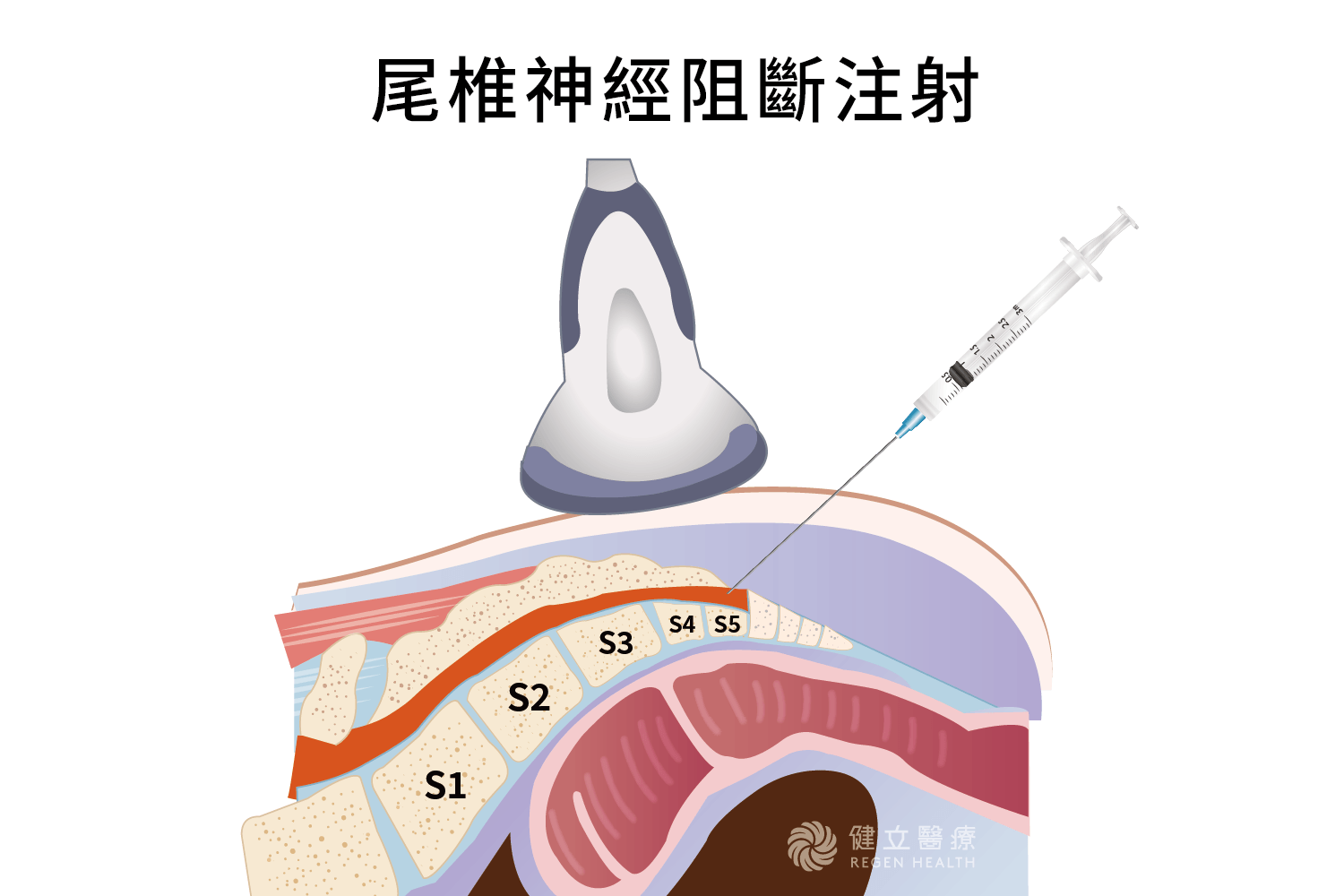
The doctor uses ultrasound or X-ray (fluorescein microscope) to precisely locate the natural foramen at the end of the coccyx—the sacral hiatus.
The needle is then inserted through this foramen, reaching below the epidural space. The injected medication (usually containing a local anesthetic and anti-inflammatory steroids) spreads upwards like irrigation, extensively covering the nerve roots in the lumbar and pelvic regions. This method effectively washes away inflammatory substances around the nerves, blocks pain transmission, and allows damaged nerves space to rest and repair.
Why choose Caudal Epidural Injection CEI? Three core advantages
1) Structural Safety: Because the needle is inserted at the lowest point of the spinal canal (where the essence of the spinal cord is stored), this is a naturally safe zone, minimizing the risk of spinal cord injury during surgery. Its safety is superior to high-level lumbar spine injections.
2) Wide Coverage: Unlike point-to-point nerve block, coccyx injections have excellent diffusion, simultaneously reaching multiple lumbosacral nerve roots, making them ideal for patients with widespread lower back pain or bilateral pain.
3) A Savior for Postoperative Pain (FBSS): If a patient has previously undergone spinal surgery, there is often severe scar tissue hyperplasia in the back, obstructing traditional injection routes. In this case, the bottom-up coccyx approach becomes an excellent alternative.
Who is suitable for Caudal Epidural Injection? (Clinical indications)
Chronic lower back pain and sciatica: Those who do not respond well to medication or physical therapy after 4-6 weeks.
Intervertebral disc degeneration or herniation: Causing radiating numbness and pain in the lower extremities.
Post-spinal surgery syndrome (FBSS): Persistent pain after surgery, or the appearance of new neuropathic symptoms. Pelvic pain: Or neuropathic pain in the lower extremities.
International medical evidence over the past decade: the practical effectiveness of Caudal Epidural Injection in clinical pain management
According to statistics from PubMed and the International Journal of Pain:
Effective Relief: Approximately 60% to 75% of patients experience a noticeable decrease in their Visual Acuity Index (VAS) and improved mobility within 1-3 months after injection.
Surgery Avoidance: Successful nerve block can help 30% to 40% of borderline surgical candidates successfully postpone or avoid surgical intervention.
Improved Accuracy: With image-guided technology, needle insertion accuracy exceeds 95%, far surpassing traditional blind injection techniques.
Interventional treatment for spinal pain: A comprehensive comparison table
| Procedure | Caudal Epidural Block | Transforaminal Epidural Injection | Analgesic injections |
|---|---|---|---|
| Injection Location |
Entering the epidural space below the coccyx through the sacral hiatus. |
Direct injection adjacent to the nerve root exit foramen |
Muscles, ligaments, or veins. |
| Safety |
Extremely high. Minimal risk of accidental injury due to its distance from the main spinal cord. |
High. Requires a highly experienced physician to avoid blood vessels and nerves. |
High. However, long-term administration may place a burden on the liver and kidneys. |
|
Treatment Logic: |
Broad irrigation from the bottom up flushes out inflammatory substances. |
Precise, targeted treatment targets a single compressed nerve. |
Systemic pain relief or relief of localized muscle tension. |
|
Suitable for: |
Widespread lower back pain, post-spinal surgery pain (FBSS), pelvic pain, acute disc herniation, severe unilateral sciatica, temporary muscle strain, and acute lower back injury. |
Acute disc herniation, severe unilateral sciatica. |
Temporary muscle strain, acute lower back injury. |
In-depth analysis: How should I choose?
1. Why is coccyx injection often called a last resort?
If you have had spinal surgery, the tissues behind your spine are usually full of scars and adhesions. In this case, injecting through the lumbar region (TF/IL) is like forcing your way through a traffic jam; the medication has difficulty spreading. Caudal Epidural injection, on the other hand, goes through the “back door” (sacral hiatus), a relatively unobstructed path, allowing the medication to easily penetrate upwards to the surgical site. It is the preferred treatment for post-spinal surgery syndrome (FBSS).
2. The decision point between “foraminal (TF)” and “coccyx (Caudal)” injections If you have pain in one leg that prevents you from walking: MRI clearly shows a herniated disc compressing a nerve. Targeted treatment via the foraminal (TF) is usually the most effective. If you have bilateral pain, deep pain in the buttocks: or if the pain is diffuse and you want the highest level of safety, the broader coverage of coccyx injection is usually more satisfying for patients.
3. From “Anti-inflammatory” to “Long-lasting Blockage” : If you’ve had a nerve block (such as a coccyx or epidural injection) that worked well but “quickly relapsed,” it means that while the inflammation is under control, the nerves may have developed chronic damage. In this case, your doctor may recommend upgrading to radiofrequency ablation (RFA), which uses a physical method to “shut down” the nerves’ response to pain signals, thus achieving a longer period of pain relief.
CEI Treatment Procedure and Frequency Recommendations
Treatment Procedure Pre-treatment Assessment:
- The doctor will assess your coagulation function (if you are taking anticoagulants such as aspirin, please inform the doctor and agree to discontinue the medication).
- Precise Localization: The patient lies prone, and the doctor uses ultrasound or X-ray for real-time guidance.
- Injection: After disinfection, the needle is inserted. The process usually only causes local tingling and numbness, and takes approximately 15-20 minutes.
Injection Frequency
This is an adjunctive treatment and will not completely cure the condition in one treatment.
- It is generally recommended to have an injection every 3 to 4 months.
- If steroids are involved, for the sake of metabolism and tissue safety, it is recommended not to exceed 3 to 4 times per year.
CEI Treatment Post-operative Precautions: 4 Key Principles for Safe Care
To ensure treatment effectiveness and prevent complications, please adhere to the following post-operative care guidelines:
- Preventing Falls (Important!): Within 12 hours post-surgery, due to the effects of anesthesia, you may experience temporary numbness or heaviness in your lower limbs. Please be supported by a family member or friend when getting out of bed.
- No Driving: Do not drive or ride a bicycle on the day of surgery. Please be picked up by a family member or friend or use public transportation to avoid accidents due to sluggish leg reflexes.
- Wound Care: Shower for 3 days post-surgery. Avoid bathing, soaking in hot springs, or swimming to prevent wound infection. If you experience mild soreness at the injection site, consult your doctor for ice pack relief.
- Physiological Monitoring: Steroids may cause temporary facial flushing, insomnia, or blood sugar fluctuations. Diabetic patients need to increase the frequency of blood sugar monitoring within three days post-surgery.
Frequently Asked Questions About Caudal Epidural Injection
Q1: Is this injection directly into the spinal cord? Will it cause paralysis?
No. The Caudal Epidural Injection route enters through the sacral hiatus, located below the end of the spinal canal. This is a treatment that avoids the main spinal cord and is extremely safe.
Q2: If I’ve had spinal surgery before, can I still have this done?
Very helpful! Scar tissue from spinal surgery is often a source of pain. The coccyx route avoids the surgical scar, allowing the medication to be distributed more effectively to the nerve compression site.
Q3: I have diabetes, is there any danger in injecting steroids?
It can be done, but strict monitoring is required. Steroids cause a temporary increase in blood sugar (usually lasting 3-5 days). As long as you follow your doctor’s instructions regarding medication adjustments and dietary monitoring after the surgery, you can usually get through this safely.
Q4: What if I’m currently taking medication to improve blood flow (anticoagulants)?
You must inform them proactively. Anticoagulants increase the risk of hematoma. Your doctor will assess your condition and determine if you need to stop taking any medication for a few days (e.g., aspirin, acetaminophen, etc.), and will only resume the treatment after confirming it is safe.
Q5: Is it normal to feel dizzy or have trouble sleeping after an injection?
Possibly. This is usually a side effect of the medication (steroids can cause excitement or metabolic fluctuations). If you experience dizziness, please sit down and rest, and avoid standing for long periods. These symptoms usually subside naturally within 24-48 hours.
Related Articles

健立醫療 目錄 Say Goodbye to Chronic, Intractable Pain! Will RF (Radiofrequency Ablation) Therapy Be Painful? Post-operative Care and 7 Frequently Asked Questions! Want to undergo RF therapy but afraid of pain or worried about the recovery period? This guide provides detailed answers to the treatment process, wound care, and 7 frequently asked questions.It helps you understand how to safely block long-term chronic pain signals through local anesthesia and minimally invasive techniques, dispelling all treatment myths and allowing you to confidently regain a pain-free life! What is Radiofrequency Ablation (RF)? Radiofrequency

Please enter a title here Regen Health Please enter a title here Is Your Shoulder Burning with Pain? Ultrasound-Guided Calcification Aspiration: Clinical Data from the Past Decade and a Comprehensive Treatment Guide Many patients are often awakened in the middle of the night or early morning by sev

Regen Health [The Complete Guide to Arthroscopic Cartilage Repair] Everything You Need to Know About the Minimally Invasive Procedure, Indications, and Postoperative Rehabilitation! Do you experience knee pain so severe that you can’t squat, feel your knee lock up after walking for a while, or even

Regen Health Say Goodbye to Joint Degeneration and Chronic Pain: A Guide to PRP Regenerative Therapy Injections, Cost Estimates, and Non-Surgical Treatment PRP (Platelet-Rich Plasma) therapy is a clinically proven, non-surgical regenerative medicine technique. By drawing approximately 10–15 cc of th

Regen Health Advanced PRP Therapy | The Golden Treatment for Activating the "Self-Repair" Mechanism of Joints and Tendons PRF is a highly safe, naturally derived regenerative medicine therapy that utilizes growth factors and fibrin structures from the patient’s own blood to help the body a

Regen Health No Hospital Stay Required! The Complete Guide to BMAC Autologous Bone Marrow Concentrate Injection Therapy When traditional regenerative therapies or hyaluronic acid fail to address severe joint degeneration, BMAC (Bone Marrow Aspirate Concentrate) offers a more advanced option. This i