Minimally Invasive De Quervain’s Release Surgery

Regen Health
2025-11-30

Minimally Invasive Release Surgery for "Mom's Hand" | Say Goodbye to Thumb and Wrist Pain and Regain Full Mobility
What Is "Mom's Hand"? (Definition of De Quervain's Syndrome)
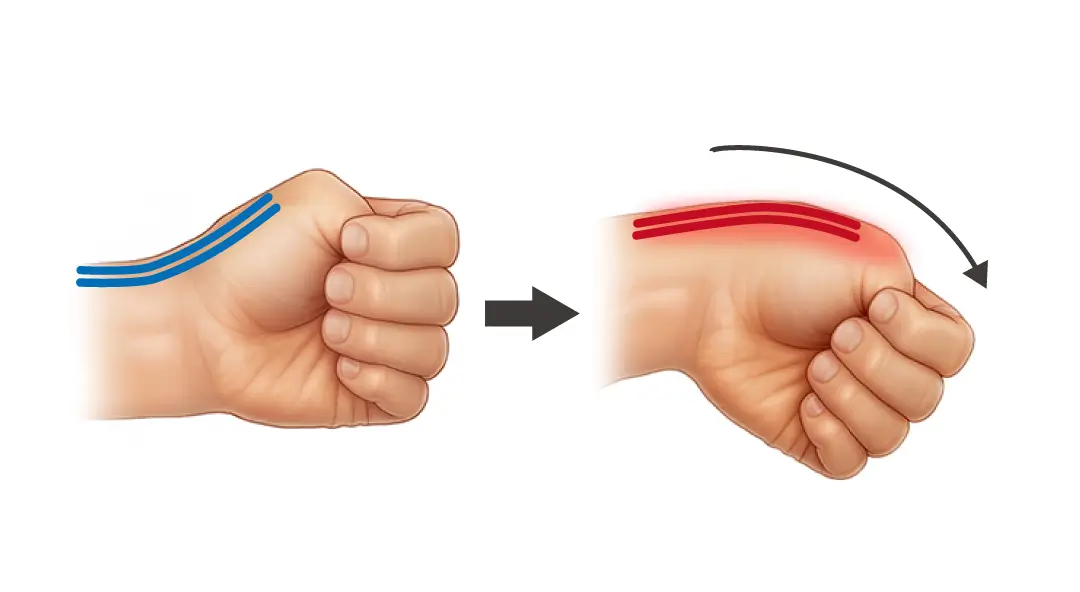
The medical term for "mom's hand" is stenosing tenosynovitis (De Quervain’s tenosynovitis), also known as De Quervain’s syndrome. This condition occurs in the "first extensor tendon sheath compartment" on the radial side (thumb side) of the wrist
.When the short abductor pollicis (EPB) and long abductor pollicis (APL) tendons experience repeated friction, causing the tendon sheath to become inflamed, swollen, and narrowed, the tendons are unable to glide smoothly, leading to severe pain and functional impairment.
The Four Main Causes of "Mom's Hand" and High-Risk Groups
Although it is commonly known as “mom’s hand,” it is not limited to new mothers; anyone who frequently uses their wrists is at risk:
- Overuse and repetitive motions: Prolonged smartphone use, typing, wringing out towels, or lifting heavy objects.
- Hormonal changes: Women during pregnancy and postpartum are at the highest risk of inflammation due to loosened connective tissue.
- Poor posture: Excessive wrist flexion when holding a baby increases the strain on the tendon sheaths.
- Tissue degeneration and variations: Older adults experience reduced tissue elasticity, or may have a congenital condition where the tendon sheath is divided into separate compartments (subcompartment variation).
Common Symptoms and Differential Diagnosis of "Mommy Wrist"
Key Symptoms
- Key Symptoms: Tenderness at the radial styloid process of the wrist; in severe cases, a hard lump may appear in the area.
- Decreased grip strength: International data indicates that the grip strength of patients with chronic carpal tunnel syndrome is, on average, approximately 25% lower than that of the healthy hand.
- Finkelstein Test: A positive result is a key indicator for diagnosis.

Differential Diagnosis (Excluding Other Causes)
- CMC Arthritis: Pain is located at the joint junction.
- Intersection Syndrome: Pain is located closer to the proximal forearm.
- Radial Nerve Compression: Often accompanied by numbness or a tingling sensation (Tinel’s sign).
Treatment Stages for De Quervain's Tenosynovitis: From Conservative Management to Minimally Invasive Surgery
1. Stage 1: Conservative Treatment (Initial Phase)
- Splinting: The injured tendon is immobilized with a splint to allow it to rest completely.
- Physical Therapy: Relieve inflammation through professional stretching and physical modalities.
- Medication and Ice Therapy: Apply ice during the acute phase to relieve pain, combined with nonsteroidal anti-inflammatory drugs (NSAIDs).
2. Phase 2: Regenerative Repair and Injection Therapy
If rest proves ineffective, advanced injection therapies may be considered:
- Prolotherapy: Injecting high-concentration glucose, PRP (Platelet-Rich Plasma), or PRF (Platelet-Rich Fibrin) to promote the tendon’s self-repair rather than merely reducing inflammation.
- Steroid Injections: While they can rapidly reduce inflammation, frequent injections may lead to tendon fragility or skin thinning.
3. Stage 3: Minimally Invasive Release Surgery for De Quervain’s Tenosynovitis (Mid-to-Late Stage / Recurrent Cases) When an “isolated
subcompartment” is present in the anatomical structure or conservative treatment has been ineffective for 3 months, minimally invasive release surgery offers a long-term solution.
Features and Benefits of Minimally Invasive Release Surgery for "Mom's Hand"
Compared to traditional open surgery, minimally invasive techniques are performed under local anesthesia and offer the following advantages:
- Small incisions, minimal trauma: Requiring only a few millimeters of incision, the procedure precisely releases the constricted tendon sheath without damaging nerves or blood vessels.
- Rapid recovery: The procedure takes approximately 15–30 minutes, and patients can resume light daily activities within a few days after surgery.
- High safety: Effectively addresses treatment challenges caused by anatomical variations (such as multiple tendons), reducing the recurrence rate.
- Minimal Discomfort: Postoperative discomfort is minimal, significantly reducing reliance on pain medication.
Clinical Data from International Journals: Evidence-Based Efficacy of Minimally Invasive Mother's Hand Release Surgery
According to studies published in leading international journals of orthopedics and hand surgery over the past decade, minimally invasive techniques have demonstrated significant advantages in the treatment of de Quervain’s tenosynovitis:
1. Optimized success and recurrence rates
- High Success Rate: According to a study published in *Archives of Orthopaedic and Trauma Surgery*, the clinical success rate of minimally invasive release surgery exceeds 95%.
2. Recovery Speed and Functional Restoration
- Visual Analogue Scale (VAS): International studies indicate that patients experience an average reduction of 70–80% in pain (VAS score) within 48 hours of undergoing minimally invasive release surgery.
- Quick Return to Work: A study in the *Journal of Hand Surgery* shows that patients who undergo minimally invasive surgery return to normal work and daily activities an average of 5.2 days earlier than those who undergo traditional open surgery.
3. Reduced Risk of Complications
- Nerve Protection: Minimally invasive techniques significantly reduce the risk of injury to the superficial radial nerve. Compared to the 3–5% risk of nerve damage associated with traditional surgery, minimally invasive techniques reduce the complication rate to less than 1%.
Prevention and Postoperative Care Recommendations for De Quervain's Tenosynovitis
- Ergonomic optimization: Adjust the keyboard height and use a mouse that fits the shape of your hand.
- Proper Baby-Holding Posture: Support the baby’s weight with the crook of your forearm to avoid excessive wrist flexion.
- Regular Stretching: Perform gentle stretching exercises for the thumb and wrist.
- Alternate Cold and Hot Compresses: Apply ice during the acute phase of redness and swelling; apply heat during the chronic phase of stiffness.
Frequently Asked Questions (FAQ) About Mom's Hand
Q1: Will "mom's hand" go away on its own?
Mild inflammation may subside with adequate rest and changes in posture; however, if you cannot stop using your hands due to work requirements, it often progresses to chronic inflammation, so early intervention is recommended.
Q2: How can I tell the difference between de Quervain’s tenosynovitis and arthritis?
The pain associated with de Quervain’s tenosynovitis is located in the “tendon sheath,” while arthritis pain is typically felt at the “base of the thumb joint (CMC).” A specialist physician will use ultrasound to accurately differentiate between the two conditions.
Q3: Is a steroid injection effective for de Quervain’s tenosynovitis?
The initial effect is significant, but it only reduces inflammation and cannot “repair” the tissue. If injections are repeated, it is recommended to switch to prolotherapy or minimally invasive surgery to protect the tendon structure.
Q4: Does minimally invasive surgery require a hospital stay?
No. This is an outpatient procedure; you can return home immediately after local anesthesia is administered, and it does not interfere with your social life.
Q5: Will the condition recur after minimally invasive release surgery?
Minimally invasive release surgery directly addresses the structural issue of "narrowing." As long as you maintain proper posture and follow the post-operative rehabilitation regimen, the chance of recurrence is extremely low.
Q6: How do I choose between ice and heat therapy?
Apply ice when the affected area feels hot, red, or painful (acute phase); apply heat when it feels tight or achy (chronic phase) to promote blood flow.
Q7: Can I receive treatment during pregnancy?
Yes. Physical therapy and orthotic support are the first-line treatments; for severe cases, consult a physician regarding safe localized treatments.
Q8: How soon after minimally invasive surgery can I return to work?
General office work can typically resume the day after surgery. If your job involves lifting heavy objects or strenuous physical labor, it is recommended to consult your doctor and wait 1–2 weeks before returning to work.
Related Articles

CASE Testimonials Popular online content creator "Goodnight Old Si Ji" suffered from recurring plantar fasciitis due to prolonged standing and constant movement, with the pain becoming so severe that he could no longer put weight on his feet. Following a professional evaluation by the orth
